

Abstract
Introduction
Malnutrition before allogeneic hematopoietic cell transplantation (allo-HCT) is known to associate with poor clinical outcome. Although various nutrition assessment tools such as subjective global assessment (SGA) and full nutritional assessment (FNA) have been used, these take a long time to evaluate and the appropriate nutrition assessment remains unclear. Controlling nutritional status (CONUT) is an easy to use tool to assess nutritional status that is estimated by laboratory information including serum albumin, total cholesterol level and total lymphocyte count (UJ Ignacio et al. 2005). CONUT is strongly correlated with SGA and FNA. We evaluated the predictive value of CONUT before allo-HCT for clinical outcome.
Methods
We retrospectively analyzed patients with myeloid malignancies who received their first allo-HCT between January 2009 and March 2017 in our institution. We evaluated the CONUT score before initiation of conditioning and compared malnutrition patients who were defined by moderate and severe score (poor CONUT group) with normal nutrition patients who were defined by normal and light score (normal CONUT group). We assessed non-relapse mortality within 100 days of allo-HCT (early NRM), disease free survival (DFS) and overall survival (OS). Comparisons between the two groups were performed using Fisher's exact test for categorical variables. The cumulative incidence of early NRM was compared using Gray's test. The probabilities of DFS and OS were estimated according to the Kaplan-Meier method and compared using the log-rank test. In the multivariate analysis, Fine and Gray's proportional-hazard model was used for the cumulative incidence of early NRM. P<0.05 were considered to be significant.
Results
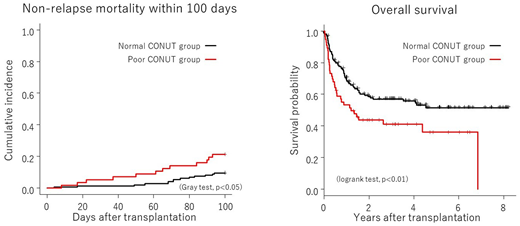
Two hundred patients were studied. The median age was 46 years (range: 17-68 years). The primary diseases were de novo AML in 106, MDS in 54, AML with Myelodysplasia-Related Changes in 30 and MDS/MPN in 10. The median CONUT score was 4 points (range: 0-12 points). Fifty-six patients were poor CONUT group and 144 patients were normal CONUT group. Age, body mass index, primary diseases, disease risk index, source of stem cell and conditioning regimen did not show significant change between the groups, while male, high HCT-CI and poor performance status patients were significantly higher in poor CONUT group (p<0.05) in patient characteristics. The total cumulative incidence of early NRM was 13.0% (26 patients, 95% CI: 8.8%-18.1%). The causes of early NRM were infection in 13, acute GVHD in 8, transplantation associated TMA in 1, interstitial pneumonia in 1, heart failure in 1, severe hepatitis in 1 and multi-organ failure in 1. The cumulative incidence of early NRM was significantly higher in the poor CONUT group than in the normal CONUT group (21.4% (95% CI: 11.8%-33.0%) versus 9.7% (95%CI: 5.6%-15.2%), p<0.05). In the multivariate analysis, the poor CONUT group was an independent significant risk factor for early NRM (HR: 2.4, 95% CI: 1.1-5.1, p<0.05). The total DFS was 56.4% at 1 year (95%CI: 49.2%-63.0%). The DFS at 1 year was significantly lower in the poor CONUT group than in the normal CONUT group (48.2% (95%CI: 34.7%-60.5%) versus 59.6% (95%CI: 51.1%-67.1%), p<0.05). The total OS was 66.0% at 1 year (95%CI: 58.9%-72.2%). The OS at 1 year was significantly lower in the poor CONUT group than the normal CONUT group (53.3% (95% CI: 39.4%-65.4%) versus 71.0% (95% CI: 62.7%-77.7%), p<0.01).
Conclusions
These findings suggested that the CONUT score before allo-HCT was a useful predictive nutrition assessment for poor survival in the patients with myeloid malignancies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal